What is the normal ECG variant? Decoding the cardiogram of the heart. How is an electrocardiogram recorded?
Electrocardiography is a method of measuring potential differences arising under the influence of electrical impulses of the heart. The result of the study is presented in the form of an electrocardiogram (ECG), which reflects the phases of the cardiac cycle and the dynamics of the heart.
During the heartbeat, the sinus node, located near the right atrium, generates electrical impulses that travel along nerve pathways, contracting the myocardium (heart muscle) of the atria and ventricles in a certain sequence.
After the myocardium contracts, the impulses continue to travel throughout the body as an electrical charge, resulting in a potential difference - a measurable value that can be determined using the electrocardiograph electrodes.
Features of the procedure
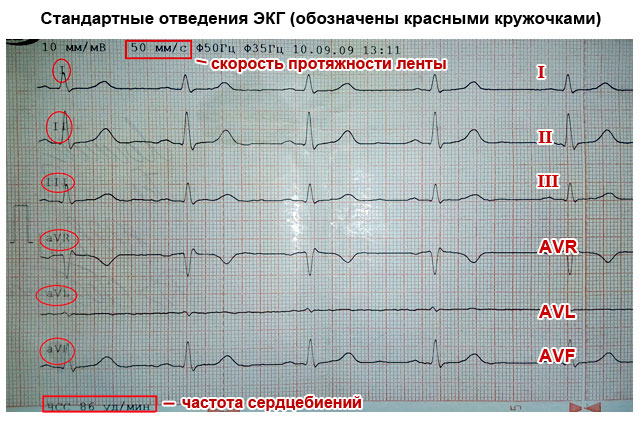
In the process of recording an electrocardiogram, leads are used - electrodes are placed according to a special scheme. To fully display the electrical potential in all parts of the heart (anterior, posterior and lateral walls, interventricular septa), 12 leads are used (three standard, three reinforced and six chest), in which electrodes are located on the arms, legs and certain areas of the chest.
During the procedure, electrodes record the strength and direction of electrical impulses, and the recording device records the resulting electromagnetic oscillations in the form of teeth and a straight line on special paper for recording ECG at a certain speed (50, 25 or 100 mm per second).
Paper registration tape uses two axes. The horizontal X axis shows time and is indicated in millimeters. Using a time period on graph paper, you can track the duration of the processes of relaxation (diastole) and contraction (systole) of all parts of the myocardium.
The vertical Y axis is an indicator of the strength of the impulses and is indicated in millivolts - mV (1 small box = 0.1 mV). By measuring the difference in electrical potentials, pathologies of the heart muscle are determined.
The ECG also shows leads, each of which alternately records the work of the heart: standard I, II, III, thoracic V1-V6 and enhanced standard aVR, aVL, aVF.
ECG indicators

The main indicators of the electrocardiogram characterizing the work of the myocardium are waves, segments and intervals.
Serrations are all sharp and rounded bumps written along the vertical Y axis, which can be positive (upward), negative (downward), or biphasic. There are five main waves that are necessarily present on the ECG graph:
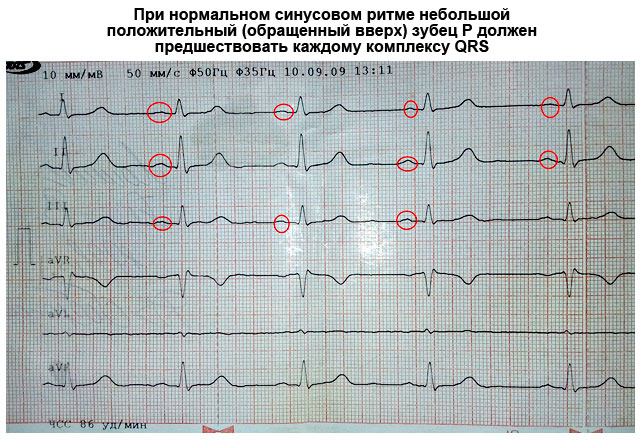
- P – recorded after the occurrence of an impulse in the sinus node and sequential contraction of the right and left atria;
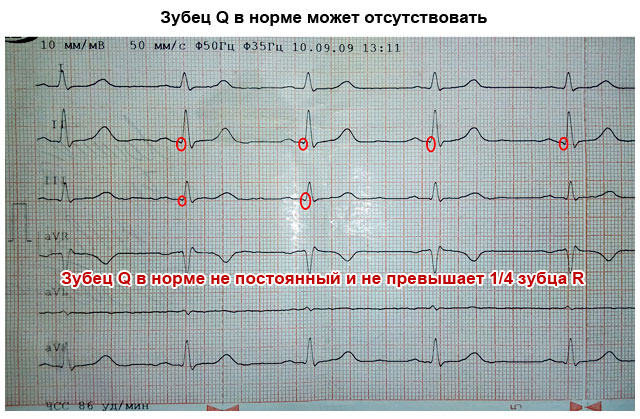
- Q – recorded when an impulse appears from the interventricular septum;
- R, S – characterize ventricular contractions;
- T - indicates the process of relaxation of the ventricles.
Segments are areas with straight lines, indicating the time of tension or relaxation of the ventricles. There are two main segments in the electrocardiogram:
- PQ – duration of ventricular excitation;
- ST – relaxation time.
An interval is a section of an electrocardiogram consisting of a wave and a segment. When studying the PQ, ST, QT intervals, the time of propagation of excitation in each atrium, in the left and right ventricles is taken into account.
ECG norm in adults (table)
Using a table of norms, you can conduct a sequential analysis of the height, intensity, shape and length of the teeth, intervals and segments to identify possible deviations. Due to the fact that the passing impulse spreads unevenly throughout the myocardium (due to the different thickness and size of the heart chambers), the main normal parameters of each element of the cardiogram are identified.
| Indicators | Norm |
|---|---|
| Prongs | |
| P | Always positive in leads I, II, aVF, negative in aVR, and biphasic in V1. Width - up to 0.12 sec, height - up to 0.25 mV (up to 2.5 mm), but in lead II the wave duration should be no more than 0.1 sec |
| Q | Q is always negative and is normally absent in leads III, aVF, V1 and V2. Duration up to 0.03 sec. Height Q: in leads I and II no more than 15% of the P wave, in III no more than 25% |
| R | Height from 1 to 24 mm |
| S | Negative. Deepest in lead V1, gradually decreases from V2 to V5, may be absent in V6 |
| T | Always positive in leads I, II, aVL, aVF, V3-V6. Always negative in aVR |
| U | Sometimes it is recorded on the cardiogram 0.04 seconds after T. The absence of U is not a pathology |
| Interval | |
| PQ | 0.12-0.20 sec |
| Complex | |
| QRS | 0.06 - 0.008 sec |
| Segment | |
| ST | In leads V1, V2, V3, it shifts upward by 2 mm |
Based on the information obtained from deciphering the ECG, conclusions can be drawn about the characteristics of the heart muscle:
- normal functioning of the sinus node;
- functioning of the conduction system;
- frequency and rhythm of heart contractions;
- the state of the myocardium – blood circulation, thickness in different areas.
ECG interpretation algorithm

There is a scheme for deciphering an ECG with a sequential study of the main aspects of heart function:
- sinus rhythm;
- rhythm regularity;
- conductivity;
- analysis of teeth and intervals.
Sinus rhythm is a uniform heartbeat rhythm caused by the appearance of an impulse in the AV node with gradual contraction of the myocardium. The presence of sinus rhythm is determined by deciphering the ECG using P wave indicators.
Also in the heart there are additional sources of excitation that regulate the heartbeat when the AV node is disturbed. Non-sinus rhythms appear on the ECG as follows:
- Atrial rhythm - P waves are below the baseline;
- AV rhythm – P is absent on the electrocardiogram or comes after the QRS complex;
- Ventricular rhythm - in the ECG there is no pattern between the P wave and the QRS complex, while the heart rate does not reach 40 beats per minute.
When the occurrence of an electrical impulse is regulated by non-sinus rhythms, the following pathologies are diagnosed:
- Extrasystole is premature contraction of the ventricles or atria. If an extraordinary P wave appears on the ECG, as well as when the polarity is deformed or changed, atrial extrasystole is diagnosed. With nodal extrasystole, P is directed downward, absent, or located between QRS and T.
- Paroxysmal tachycardia (140-250 beats per minute) on the ECG can be presented in the form of an overlay of the P wave on the T wave, standing behind the QRS complex in standard leads II and III, as well as in the form of an extended QRS.
- Flutter (200-400 beats per minute) of the ventricles is characterized by high waves with difficult to distinguish elements, and with atrial flutter, only the QRS complex is distinguished, and sawtooth waves are present in place of the P wave.
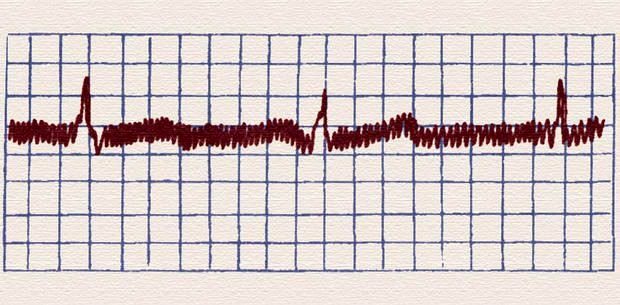
- Flicker (350-700 beats per minute) on the ECG is expressed in the form of inhomogeneous waves.
Heart rate
The interpretation of the ECG of the heart must contain heart rate indicators and is recorded on tape. To determine the indicator, you can use special formulas depending on the recording speed:
- at a speed of 50 millimeters per second: 600/ (number of large squares in the R-R interval);
- at a speed of 25 mm per second: 300/ (number of large squares between R-R),
Also, the numerical indicator of the heartbeat can be determined by the small cells of the R-R interval, if the ECG tape was recorded at a speed of 50 mm/s:
- 3000/number of small cells.
The normal heart rate for an adult is between 60 and 80 beats per minute.
Regularity of rhythm
Normally, the R-R intervals are the same, but an increase or decrease of no more than 10% from the average value is allowed. Changes in the regularity of the rhythm and increased/decreased heart rate can occur as a result of disturbances in automatism, excitability, conductivity, and contractility of the myocardium.
When the automatic function is impaired, the following interval indicators are observed in the heart muscle:
- tachycardia - heart rate is in the range of 85-140 beats per minute, a short period of relaxation (TP interval) and a short RR interval;
- bradycardia - heart rate decreases to 40-60 beats per minute, and the distances between RR and TP increase;
- arrhythmia – different distances are tracked between the main heartbeat intervals.
Conductivity
To quickly transmit an impulse from the source of excitation to all parts of the heart, there is a special conduction system (SA and AV nodes, as well as the His bundle), the violation of which is called blockade.
There are three main types of blockades - sinus, intraatrial and atrioventricular.
With sinus block, the ECG shows a violation of impulse transmission to the atria in the form of periodic loss of PQRST cycles, while the distance between R-R increases significantly.
Intraatrial block is expressed as a long P wave (more than 0.11 s).
Atrioventricular block is divided into several degrees:
- I degree – prolongation of the P-Q interval by more than 0.20 s;
- II degree - periodic loss of QRST with an uneven change in time between complexes;
- III degree - the ventricles and atria contract independently of each other, as a result of which there is no connection between P and QRST in the cardiogram.
Electric axis
EOS displays the sequence of impulse transmission through the myocardium and normally can be horizontal, vertical and intermediate. In ECG interpretation, the electrical axis of the heart is determined by the location of the QRS complex in two leads - aVL and aVF.
In some cases, axis deviation occurs, which in itself is not a disease and occurs due to an enlargement of the left ventricle, but, at the same time, may indicate the development of pathologies of the heart muscle. As a rule, the EOS deviates to the left due to:
- ischemic syndrome;
- pathology of the valve apparatus of the left ventricle;
- arterial hypertension.
A tilt of the axis to the right is observed with enlargement of the right ventricle with the development of the following diseases:
- pulmonary stenosis;
- bronchitis;
- asthma;
- pathology of the tricuspid valve;
- congenital defect.
Deviations
Violations in the duration of intervals and wave heights are also signs of changes in the functioning of the heart, on the basis of which a number of congenital and acquired pathologies can be diagnosed.
| ECG indicators | Possible pathologies |
|---|---|
| P wave | |
| Pointed, greater than 2.5 mV | Congenital defect, coronary artery disease, congestive heart failure |
| Negative in lead I | Septal defects, pulmonary stenosis |
| Deep negative in V1 | Heart failure, myocardial infarction, mitral, aortic valve disease |
| P-Q interval | |
| Less than 0.12 s | Hypertension, vasoconstriction |
| More than 0.2 s | Atrioventricular block, pericarditis, infarction |
| QRST waves | |
| In lead I and aVL there is a low R and deep S, as well as a small Q in the lead. II, III, aVF | Right ventricular hypertrophy, lateral myocardial infarction, vertical position of the heart |
| Late R in hole. V1-V2, deep S in hole. I, V5-V6, negative T | Ischemic disease, Lenegra disease |
| Wide serrated R in hole. I, V5-V6, deep S in hole. V1-V2, absence of Q in hole. I, V5-V6 | Left ventricular hypertrophy, myocardial infarction |
| Voltage below normal | Pericarditis, protein metabolism disorder, hypothyroidism |
From this article you will learn about such a diagnostic method as an ECG of the heart - what it is and what it shows. How an electrocardiogram is recorded, and who can most accurately decipher it. You will also learn how to independently determine the signs of a normal ECG and major heart diseases that can be diagnosed using this method.
Article publication date: 03/02/2017
Article updated date: 05/29/2019
What is an ECG (electrocardiogram)? This is one of the simplest, most accessible and informative methods for diagnosing heart disease. It is based on recording electrical impulses arising in the heart and graphically recording them in the form of teeth on a special paper film.
Based on these data, one can judge not only the electrical activity of the heart, but also the structure of the myocardium. This means that an ECG can diagnose many different heart conditions. Therefore, independent interpretation of the ECG by a person who does not have special medical knowledge is impossible.
All that an ordinary person can do is only roughly assess the individual parameters of the electrocardiogram, whether they correspond to the norm and what pathology they may indicate. But final conclusions based on the ECG conclusion can only be made by a qualified specialist - a cardiologist, as well as a therapist or family doctor.
Principle of the method
The contractile activity and functioning of the heart is possible due to the fact that spontaneous electrical impulses (discharges) regularly occur in it. Normally, their source is located in the uppermost part of the organ (in the sinus node, located near the right atrium). The purpose of each impulse is to travel along the nerve pathways through all parts of the myocardium, causing them to contract. When an impulse arises and passes through the myocardium of the atria and then the ventricles, their alternating contraction occurs - systole. During the period when there are no impulses, the heart relaxes - diastole.
ECG diagnostics (electrocardiography) is based on recording electrical impulses arising in the heart. For this purpose, a special device is used - an electrocardiograph. The principle of its operation is to capture on the surface of the body the difference in bioelectric potentials (discharges) that occur in different parts of the heart at the moment of contraction (in systole) and relaxation (in diastole). All these processes are recorded on special heat-sensitive paper in the form of a graph consisting of pointed or hemispherical teeth and horizontal lines in the form of spaces between them.

What else is important to know about electrocardiography
Electrical discharges of the heart pass not only through this organ. Since the body has good electrical conductivity, the strength of the exciting cardiac impulses is sufficient to pass through all tissues of the body. They spread best to the chest in the area, as well as to the upper and lower extremities. This feature is the basis of the ECG and explains what it is.
In order to record the electrical activity of the heart, it is necessary to fix one electrocardiograph electrode on the arms and legs, as well as on the anterolateral surface of the left half of the chest. This allows you to capture all directions of electrical impulses propagating throughout the body. The paths of discharges between the areas of contraction and relaxation of the myocardium are called cardiac leads and are designated on the cardiogram as follows:
- Standard leads:
- I – first;
- II – second;
- Ш – third;
- AVL (analogue of the first);
- AVF (analogue of the third);
- AVR (mirroring all leads).
The significance of the leads is that each of them registers the passage of an electrical impulse through a certain area of the heart. Thanks to this, you can obtain information about:
- How the heart is located in the chest (the electrical axis of the heart, which coincides with the anatomical axis).
- What is the structure, thickness and nature of blood circulation of the myocardium of the atria and ventricles.
- How regularly do impulses occur in the sinus node and are there any interruptions?
- Are all impulses carried out along the paths of the conducting system, and are there any obstacles in their path?
What does an electrocardiogram consist of?
If the heart had the same structure of all its departments, nerve impulses would pass through them in the same time. As a result, on the ECG, each electrical discharge would correspond to only one tooth, which reflects the contraction. The period between contractions (impulses) on the EGC looks like an even horizontal line, which is called an isoline.
The human heart consists of right and left halves, in which the upper part is the atria, and the lower part is the ventricles. Since they have different sizes, thicknesses and are separated by partitions, the exciting impulse passes through them at different speeds. Therefore, different waves corresponding to a specific part of the heart are recorded on the ECG.
What do the teeth mean?
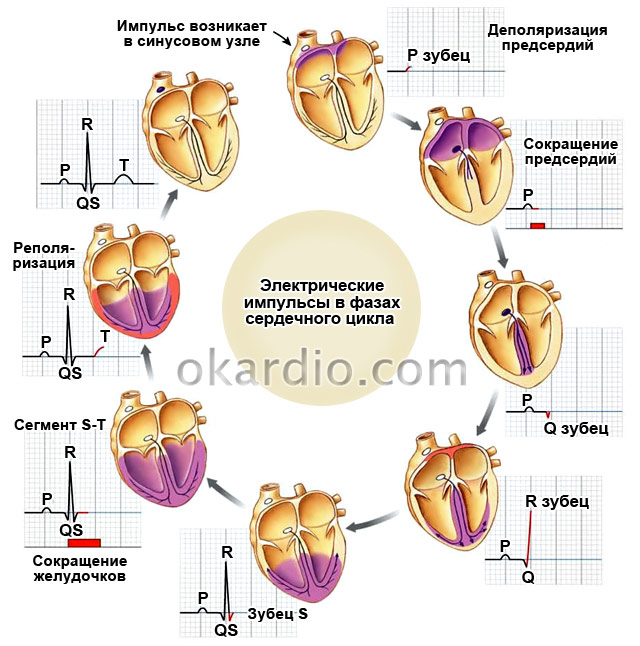
The sequence of propagation of systolic excitation of the heart is as follows:
- The origin of electric pulse discharges occurs in the sinus node. Since it is located close to the right atrium, it is this section that contracts first. With a slight delay, almost simultaneously, the left atrium contracts. On the ECG, such a moment is reflected by the P wave, which is why it is called atrial. It faces up.
- From the atria, the discharge passes to the ventricles through the atrioventricular (atrioventricular) node (a collection of modified myocardial nerve cells). They have good electrical conductivity, so delays in the node do not normally occur. This is displayed on the ECG as the P-Q interval - a horizontal line between the corresponding teeth.
- Excitation of the ventricles. This part of the heart has the thickest myocardium, so the electrical wave travels through them longer than through the atria. As a result, the highest wave appears on the ECG - R (ventricular), facing upward. It may be preceded by a small Q wave, the apex of which faces in the opposite direction.
- After the completion of ventricular systole, the myocardium begins to relax and restore energy potentials. On the ECG it looks like an S wave (facing down) - a complete lack of excitability. After it comes a small T wave, facing upward, preceded by a short horizontal line - the S-T segment. They indicate that the myocardium has fully recovered and is ready to make another contraction.

Since each electrode attached to the limbs and chest (lead) corresponds to a specific part of the heart, the same teeth look different in different leads - they are more pronounced in some, and less in others.
How to decipher a cardiogram
Sequential ECG interpretation in both adults and children involves measuring the size, length of the waves and intervals, assessing their shape and direction. Your actions with decryption should be as follows:
- Unfold the paper with the recorded ECG. It can be either narrow (about 10 cm) or wide (about 20 cm). You will see several jagged lines running horizontally, parallel to each other. After a short interval in which there are no teeth, after the recording is interrupted (1–2 cm), the line with several complexes of teeth begins again. Each such graph displays a lead, so it is preceded by a designation of which lead it is (for example, I, II, III, AVL, V1, etc.).
- In one of the standard leads (I, II or III) in which the R wave is the highest (usually the second), measure the distance between three successive R waves (R-R-R interval) and determine the average value (divide number of millimeters per 2). This is necessary to calculate the heart rate per minute. Remember that these and other measurements can be made with a millimeter ruler or by calculating the distance using an ECG tape. Each large cell on the paper corresponds to 5 mm, and each dot or small cell inside it corresponds to 1 mm.
- Assess the spaces between the R waves: are they the same or different? This is necessary in order to determine the regularity of the heart rhythm.
- Sequentially evaluate and measure each wave and interval on the ECG. Determine their compliance with normal indicators (table below).

Important to remember! Always pay attention to the speed of the tape - 25 or 50 mm per second. This is fundamentally important for calculating heart rate (HR). Modern devices indicate heart rate on a tape, and there is no need to count.
How to count your heart rate
There are several ways to count the number of heartbeats per minute:
- Typically, the ECG is recorded at a speed of 50 mm/sec. In this case, you can calculate your heart rate (heart rate) using the following formulas:
Heart rate=60/((R-R (in mm)*0.02))
When recording an ECG at a speed of 25 mm/sec:
Heart rate=60/((R-R (in mm)*0.04)
- You can also calculate the heart rate on a cardiogram using the following formulas:
- When recording at 50 mm/sec: HR = 600/average number of large cells between R waves.
- When recording at 25 mm/sec: HR = 300/average of the number of large cells between the R waves.

What does an ECG look like normally and with pathology?
What a normal ECG and wave complexes should look like, what deviations occur most often and what they indicate are described in the table.
Important to remember!
- One small cell (1 mm) on the ECG film corresponds to 0.02 seconds when recording at 50 mm/sec and 0.04 seconds when recording at 25 mm/sec (for example, 5 cells - 5 mm - one large cell corresponds to 1 second).
- The AVR lead is not used for evaluation. Normally, it is a mirror image of standard leads.
- The first lead (I) duplicates the AVL, and the third (III) duplicates the AVF, so they look almost identical on the ECG.

| ECG parameters | Normal indicators | How to decipher deviations from the norm on a cardiogram, and what they indicate |
|---|---|---|
| Distance R–R–R | All spaces between R waves are equal | Different intervals may indicate atrial fibrillation, heart block |
| Heart rate | In the range from 60 to 90 beats/min | Tachycardia – when heart rate is more than 90/min Bradycardia – less than 60/min |
| P wave (atrial contraction) | Facing upward like an arc, about 2 mm high, precedes each R wave. May be absent in III, V1 and AVL | High (more than 3 mm), wide (more than 5 mm), in the form of two halves (double-humped) - thickening of the atrial myocardium |
| Generally absent in leads I, II, FVF, V2 – V6 – the rhythm does not come from the sinus node | ||
| Several small sawtooth-shaped teeth between the R waves – atrial fibrillation | ||
| P–Q interval | Horizontal line between P and Q waves 0.1–0.2 seconds | If it is elongated (more than 1 cm when recording 50 mm/sec) – hearts |
| Shortening (less than 3 mm) – | ||
| QRS complex | Duration is about 0.1 sec (5 mm), after each complex there is a T wave and there is a horizontal line gap | Expansion of the ventricular complex indicates hypertrophy of the ventricular myocardium, bundle branch block |
| If there are no gaps between high complexes facing upward (they go continuously), this indicates either ventricular fibrillation | ||
| Looks like a “flag” – myocardial infarction | ||
| Q wave | Downward facing, less than ¼ R deep, may be absent | A deep and wide Q wave in standard or precordial leads indicates acute or previous myocardial infarction |
| R wave | The highest, facing upward (about 10–15 mm), pointed, present in all leads | It may have different heights in different leads, but if it is more than 15–20 mm in leads I, AVL, V5, V6, this may indicate. A jagged R at the top in the shape of the letter M indicates a bundle branch block. |
| S wave | Available in all leads, facing down, pointed, can have different depths: 2–5 mm in standard leads | Normally, in the chest leads its depth can be as many millimeters as the height R, but should not exceed 20 mm, and in leads V2–V4 the depth of S is the same as the height of R. Deep or jagged S in III, AVF, V1, V2 – left ventricular hypertrophy. |
| Segment S–T | Corresponds to the horizontal line between the S and T waves | Deviation of the electrocardiographic line up or down from the horizontal plane by more than 2 mm indicates coronary artery disease, angina pectoris or myocardial infarction |
| T wave | Facing upwards in the form of an arc with a height of less than ½ R, in V1 it can have the same height, but should not be higher | A tall, pointed, double-humped T in the standard and chest leads indicates coronary disease and heart overload |
| The T wave merging with the S–T interval and the R wave in the form of an arcuate “flag” indicates an acute period of infarction |


Something else important
The ECG characteristics described in the table in normal and pathological conditions are only a simplified version of the decoding. A full assessment of the results and the correct conclusion can only be made by a specialist (cardiologist) who knows the extended scheme and all the intricacies of the method. This is especially true when you need to decipher an ECG in children. The general principles and elements of the cardiogram are the same as for adults. But there are different standards for children of different ages. Therefore, only pediatric cardiologists can make a professional assessment in controversial and doubtful cases.
ECG (electrocardiography, or simply, cardiogram) is the main method for studying cardiac activity. The method is so simple, convenient, and, at the same time, informative that it is used everywhere. In addition, ECG is absolutely safe, and there are no contraindications to it.
Therefore, it is used not only for diagnosing cardiovascular diseases, but also as a preventive measure during routine medical examinations and before sports competitions. In addition, ECG is recorded to determine suitability for certain professions associated with heavy physical activity.
Our heart contracts under the influence of impulses that pass through the conduction system of the heart. Each pulse represents an electrical current. This current originates at the point where the impulse is generated in the sinus node, and then goes to the atria and ventricles. Under the influence of the impulse, contraction (systole) and relaxation (diastole) of the atria and ventricles occurs.
Moreover, systole and diastole occur in strict sequence - first in the atria (in the right atrium a little earlier), and then in the ventricles. This is the only way to ensure normal hemodynamics (blood circulation) with a complete blood supply to organs and tissues.
Electric currents in the conduction system of the heart create an electric and magnetic field around itself. One of the characteristics of this field is electric potential. With abnormal contractions and inadequate hemodynamics, the magnitude of the potentials will differ from the potentials characteristic of cardiac contractions of a healthy heart. In any case, both normally and in pathology, the electrical potentials are negligibly small.
But tissues have electrical conductivity, and therefore the electric field of a beating heart spreads throughout the body, and potentials can be recorded on the surface of the body. All that is needed for this is a highly sensitive apparatus equipped with sensors or electrodes. If, with the help of this device, called an electrocardiograph, electrical potentials corresponding to the impulses of the conduction system are recorded, then one can judge the functioning of the heart and diagnose disorders of its functioning.
This idea formed the basis of the corresponding concept developed by the Dutch physiologist Einthoven. At the end of the 19th century. this scientist formulated the basic principles of ECG and created the first cardiograph. In a simplified form, an electrocardiograph consists of electrodes, a galvanometer, an amplification system, lead switches, and a recording device. Electrical potentials are sensed by electrodes that are placed on various parts of the body. The lead is selected using the device switch.
Since the electrical potentials are negligibly small, they are first amplified and then applied to the galvanometer, and from there, in turn, to the recording device. This device is an ink recorder and a paper tape. Already at the beginning of the 20th century. Einthoven was the first to use ECG for diagnostic purposes, for which he was awarded the Nobel Prize.
ECG Triangle of Einthoven
According to Einthoven's theory, the human heart, located in the chest with a shift to the left, is in the center of a kind of triangle. The vertices of this triangle, which is called the Einthoven triangle, are formed by three limbs - the right arm, the left arm, and the left leg. Einthoven proposed recording the potential difference between electrodes placed on the limbs.
The potential difference is determined in three leads, which are called standard leads and are designated by Roman numerals. These leads are the sides of Einthoven's triangle. Moreover, depending on the lead in which the ECG is recorded, the same electrode can be active, positive (+), or negative (-):
- Left hand (+) – right hand (-)
- Right hand (-) – left leg (+)
- Left arm (-) – left leg (+)
Rice. 1. Einthoven's triangle.
A little later, it was proposed to register enhanced unipolar leads from the limbs - the apices of Eythoven's triangle. These enhanced leads are designated by the English abbreviations aV (augmented voltage).
aVL (left) – left hand;
aVR (right) – right hand;
aVF (foot) – left leg.
In enhanced unipolar leads, the potential difference is determined between the limb on which the active electrode is applied and the average potential of the other two limbs.
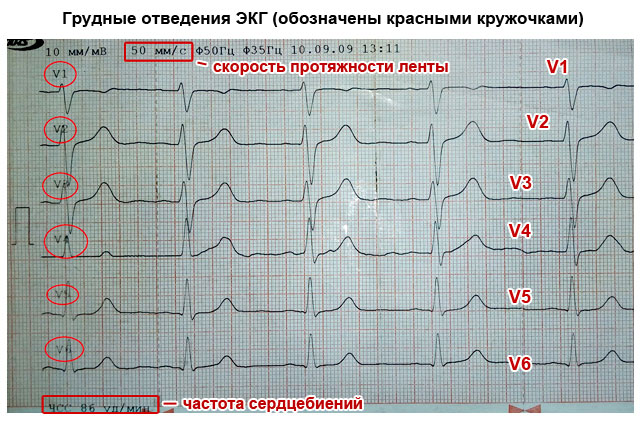
In the middle of the 20th century. The ECG was supplemented by Wilson, who, in addition to standard and unipolar leads, proposed recording the electrical activity of the heart from unipolar chest leads. These leads are designated by the letter V. For ECG studies, six unipolar leads are used, located on the anterior surface of the chest.
Since cardiac pathology usually affects the left ventricle of the heart, most chest leads V are located in the left half of the chest.

Rice. 2.
V 1 – fourth intercostal space at the right edge of the sternum;
V 2 – fourth intercostal space at the left edge of the sternum;
V 3 – the middle between V 1 and V 2;
V 4 – fifth intercostal space along the midclavicular line;
V 5 – horizontally along the anterior axillary line at the level of V 4;
V 6 – horizontally along the midaxillary line at the level of V 4.
These 12 leads (3 standard + 3 unipolar from the limbs + 6 chest) are mandatory. They are recorded and assessed in all cases of ECG performed for diagnostic or preventive purposes.
In addition, there are a number of additional leads. They are recorded rarely and for certain indications, for example, when it is necessary to clarify the localization of myocardial infarction, to diagnose hypertrophy of the right ventricle, atria, etc. Additional ECG leads include chest leads:
V 7 – at the level of V 4 -V 6 along the posterior axillary line;
V 8 – at the level of V 4 -V 6 along the scapular line;
V 9 – at the level of V 4 -V 6 along the paravertebral (paravertebral) line.
In rare cases, to diagnose changes in the upper parts of the heart, chest electrodes may be placed 1-2 intercostal spaces higher than usual. In this case, they are denoted by V 1, V 2, where the superscript indicates how many intercostal spaces the electrode is located above.
Sometimes, to diagnose changes in the right side of the heart, chest electrodes are applied to the right half of the chest at points that are symmetrical to those with the standard method of recording chest leads in the left half of the chest. In the designation of such leads, the letter R is used, which means right, right - B 3 R, B 4 R.
Cardiologists sometimes resort to bipolar leads, once proposed by the German scientist Neb. The principle of registering leads according to the Sky is approximately the same as registering standard leads I, II, III. But in order to form a triangle, electrodes are placed not on the limbs, but on the chest.
An electrode from the right hand is installed in the second intercostal space at the right edge of the sternum, from the left hand - along the posterior axillary line at the level of the actuator of the heart, and from the left leg - directly to the projection point of the actuator of the heart, corresponding to V 4. Between these points, three leads are recorded, which are designated by the Latin letters D, A, I:
D (dorsalis) – posterior lead, corresponds to standard lead I, similar to V 7;
A (anterior) – anterior lead, corresponds to standard lead II, similar to V 5;
I (inferior) – inferior lead, corresponds to standard lead III, similar to V 2.
To diagnose posterobasal forms of infarction, Slopak leads are registered, designated by the letter S. When registering Slopak leads, the electrode placed on the left arm is installed along the left posterior axillary line at the level of the apical impulse, and the electrode from the right arm is moved alternately to four points:
S 1 – at the left edge of the sternum;
S 2 – along the midclavicular line;
S 3 – in the middle between C 2 and C 4;
S 4 – along the anterior axillary line.
In rare cases, for ECG diagnostics, precordial mapping is used, when 35 electrodes in 5 rows of 7 each are located on the left anterolateral surface of the chest. Sometimes the electrodes are placed in the epigastric region, advanced into the esophagus at a distance of 30-50 cm from the incisors, and even inserted into the cavity of the heart chambers when probing it through large vessels. But all these specific methods of ECG registration are carried out only in specialized centers that have the necessary equipment and qualified doctors.
ECG technique
As planned, ECG recording is carried out in a specialized room equipped with an electrocardiograph. Some modern cardiographs use a thermal printing mechanism instead of a conventional ink recorder, which uses heat to burn the cardiogram curve onto the paper. But in this case, the cardiogram requires special paper or thermal paper. For clarity and convenience of calculating ECG parameters, cardiographs use graph paper.
In the latest modifications of cardiographs, the ECG is displayed on the monitor screen, decrypted using the supplied software, and not only printed on paper, but also saved on digital media (disk, flash drive). Despite all these improvements, the principle of the ECG recording cardiograph has remained virtually unchanged since Einthoven developed it.
Most modern electrocardiographs are multichannel. Unlike traditional single-channel devices, they record not one, but several leads at once. In 3-channel devices, first standard I, II, III are recorded, then enhanced unipolar leads from the limbs aVL, aVR, aVF, and then chest leads - V 1-3 and V 4-6. In 6-channel electrocardiographs, standard and unipolar limb leads are first recorded, and then all chest leads.
The room in which recording is carried out must be removed from sources of electromagnetic fields and X-ray radiation. Therefore, the ECG room should not be placed in close proximity to the X-ray room, rooms where physiotherapeutic procedures are carried out, as well as electric motors, power panels, cables, etc.
There is no special preparation before recording an ECG. It is advisable for the patient to be rested and well-slept. Previous physical and psycho-emotional stress can affect the results and is therefore undesirable. Sometimes food intake can also affect the results. Therefore, an ECG is recorded on an empty stomach, no earlier than 2 hours after a meal.
While recording an ECG, the subject lies on a flat, hard surface (on a couch) in a relaxed state. Places for applying electrodes must be free of clothing.
Therefore, you need to undress to the waist, free your shins and feet from clothes and shoes. Electrodes are applied to the inner surfaces of the lower thirds of the legs and feet (the inner surface of the wrist and ankle joints). These electrodes have the form of plates and are designed for recording standard leads and unipolar leads from the limbs. These same electrodes may look like bracelets or clothespins.
In this case, each limb has its own electrode. To avoid errors and confusion, the electrodes or wires through which they are connected to the device are color coded:
- To the right hand - red;
- To the left hand - yellow;
- To the left leg - green;
- To the right leg - black.
Why do you need a black electrode? After all, the right leg is not included in the Einthoven triangle, and readings are not taken from it. The black electrode is for grounding. According to basic safety requirements, all electrical equipment, incl. and electrocardiographs must be grounded.
For this purpose, ECG rooms are equipped with a grounding circuit. And if the ECG is recorded in a non-specialized room, for example, at home by ambulance workers, the device is grounded to a central heating radiator or to a water pipe. For this there is a special wire with a fixing clip at the end.
Electrodes for recording chest leads have the shape of a suction cup and are equipped with a white wire. If the device is single-channel, there is only one suction cup, and it is moved to the required points on the chest.
In multi-channel devices there are six of these suction cups, and they are also marked with color:
V 1 – red;
V 2 – yellow;
V 3 – green;
V 4 – brown;
V 5 – black;
V 6 – purple or blue.
It is important that all electrodes adhere tightly to the skin. The skin itself should be clean, free of oil, fat and sweat. Otherwise, the quality of the electrocardiogram may deteriorate. Inductive currents, or simply interference, arise between the skin and the electrode. Quite often, the tip occurs in men with thick hair on the chest and limbs. Therefore, here you need to be especially careful to ensure that the contact between the skin and the electrode is not broken. The interference sharply worsens the quality of the electrocardiogram, which displays small teeth instead of a straight line.
Rice. 3. Induced currents.
Therefore, it is recommended to degrease the area where the electrodes are applied with alcohol and moisten it with a soap solution or conductive gel. For electrodes from the limbs, gauze wipes soaked in saline solution are also suitable. However, it should be borne in mind that the saline solution dries quickly and the contact may be broken.
Before recording, it is necessary to check the calibration of the device. For this purpose, it has a special button - the so-called. reference millivolt. This value reflects the height of the tooth at a potential difference of 1 millivolt (1 mV). In electrocardiography, the reference millivolt value is 1 cm. This means that with a difference in electrical potentials of 1 mV, the height (or depth) of the ECG wave is 1 cm.
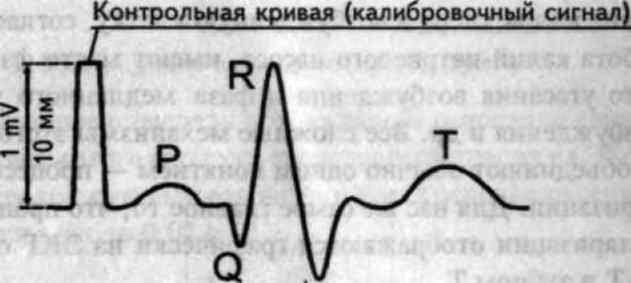
Rice. 4. Each ECG recording must be preceded by a control millivolt test.
Electrocardiograms are recorded at a tape speed of 10 to 100 mm/s. True, extreme values are used very rarely. Basically, the cardiogram is recorded at a speed of 25 or 50 mm/s. Moreover, the last value, 50 mm/s, is standard and most often used. A speed of 25 mm/h is used where the greatest number of heart contractions needs to be recorded. After all, the lower the speed of the tape, the greater the number of heart contractions it displays per unit of time.
Rice. 5. The same ECG recorded at a speed of 50 mm/s and 25 mm/s.
An ECG is recorded during quiet breathing. In this case, the subject should not talk, sneeze, cough, laugh, or make sudden movements. When registering standard lead III, a deep breath with a short breath hold may be required. This is done in order to distinguish functional changes, which are often found in this lead, from pathological ones.
The section of the cardiogram with teeth corresponding to the systole and diastole of the heart is called the cardiac cycle. Typically, 4-5 cardiac cycles are recorded in each lead. In most cases this is enough. However, in case of cardiac arrhythmias or suspected myocardial infarction, recording up to 8-10 cycles may be required. To switch from one lead to another, the nurse uses a special switch.
At the end of the recording, the subject is released from the electrodes, and the tape is signed - their full name is indicated at the very beginning. and age. Sometimes, to detail the pathology or determine physical endurance, an ECG is performed against the background of medication or physical activity. Drug tests are carried out with various drugs - atropine, chimes, potassium chloride, beta-blockers. Physical activity is carried out on an exercise bike (bicycle ergometry), walking on a treadmill, or walking for certain distances. To ensure completeness of information, an ECG is recorded before and after exercise, as well as directly during bicycle ergometry.
Many negative changes in heart function, such as rhythm disturbances, are transient and may not be detected during ECG recording even with a large number of leads. In these cases, Holter monitoring is performed - a Holter ECG is recorded in continuous mode throughout the day. A portable recorder equipped with electrodes is attached to the patient's body. Then the patient goes home, where he follows his usual routine. After 24 hours, the recording device is removed and the available data is decrypted.
A normal ECG looks something like this:
Rice. 6. ECG tape
All deviations in the cardiogram from the midline (isoline) are called waves. Teeth deviated upward from the isoline are considered to be positive, and downward - negative. The space between the teeth is called a segment, and the tooth and its corresponding segment are called an interval. Before finding out what a particular wave, segment or interval represents, it is worth briefly dwelling on the principle of forming an ECG curve.
Normally, the cardiac impulse originates in the sinoatrial (sinus) node of the right atrium. Then it spreads to the atria - first the right, then the left. After this, the impulse is sent to the atrioventricular node (atrioventricular or AV junction), and then along the His bundle. The branches of the His bundle or pedicles (right, left anterior and left posterior) end in Purkinje fibers. From these fibers, the impulse propagates directly to the myocardium, leading to its contraction - systole, which is replaced by relaxation - diastole.
The passage of an impulse along a nerve fiber and the subsequent contraction of the cardiomyocyte is a complex electromechanical process, during which the values of the electrical potentials on both sides of the fiber membrane change. The difference between these potentials is called the transmembrane potential (TMP). This difference is due to the different permeability of the membrane to potassium and sodium ions. There is more potassium inside the cell, sodium - outside it. As the pulse passes, this permeability changes. In the same way, the ratio of intracellular potassium and sodium and TMP changes.
When an excitatory impulse passes, TMP increases inside the cell. In this case, the isoline shifts upward, forming the ascending part of the tooth. This process is called depolarization. Then, after the passage of the pulse, the TMP tries to take the original value. However, the permeability of the membrane to sodium and potassium does not immediately return to normal and takes some time.
This process, called repolarization, is manifested on the ECG by a downward deviation of the isoline and the formation of a negative wave. Then the polarization of the membrane takes on the initial resting value (TMP), and the ECG again takes on the character of an isoline. This corresponds to the diastole phase of the heart. It is noteworthy that the same tooth can look both positive and negative. It all depends on the projection, i.e. the lead in which it is recorded.
ECG components
ECG waves are usually designated in Latin capital letters, starting with the letter P.

Rice. 7. ECG waves, segments and intervals.
The parameters of the teeth are direction (positive, negative, two-phase), as well as height and width. Since the height of the tooth corresponds to the change in potential, it is measured in mV. As already mentioned, a height of 1 cm on the tape corresponds to a potential deviation of 1 mV (reference millivolt). The width of a tooth, segment or interval corresponds to the duration of a phase of a particular cycle. This is a temporary value, and it is customary to denote it not in millimeters, but in milliseconds (ms).
When the tape moves at a speed of 50 mm/s, each millimeter on paper corresponds to 0.02 s, 5 mm - 0.1 ms, and 1 cm - 0.2 ms. It's very simple: if 1 cm or 10 mm (distance) is divided by 50 mm/s (speed), we get 0.2 ms (time).
Prong R. Displays the spread of excitation throughout the atria. In most leads it is positive, and its height is 0.25 mV and width is 0.1 ms. Moreover, the initial part of the wave corresponds to the passage of the impulse through the right ventricle (since it is excited earlier), and the final part - along the left. The P wave may be negative or biphasic in leads III, aVL, V 1, and V 2.
Interval P-Q (orP-R)- the distance from the beginning of the P wave to the beginning of the next wave - Q or R. This interval corresponds to the depolarization of the atria and the passage of the impulse through the AV junction, and then along the His bundle and its legs. The size of the interval depends on the heart rate (HR) - the higher it is, the shorter the interval. Normal values are in the range of 0.12 – 0.2 ms. A wide interval indicates a slowdown in atrioventricular conduction.
Complex QRS. If P represents the functioning of the atria, then the following waves, Q, R, S and T, reflect the function of the ventricles, and correspond to the various phases of depolarization and repolarization. The set of QRS waves is called the ventricular QRS complex. Normally, its width should be no more than 0.1 ms. An excess indicates a violation of intraventricular conduction.
Prong Q. Corresponds to depolarization of the interventricular septum. This tooth is always negative. Normally, the width of this wave does not exceed 0.3 ms, and its height is no more than ¼ of the next R wave in the same lead. The only exception is lead aVR, where a deep Q wave is recorded. In other leads, a deep and widened Q wave (in medical slang - kuishche) may indicate a serious heart pathology - acute myocardial infarction or scars after a heart attack. Although other reasons are possible - deviations of the electrical axis due to hypertrophy of the heart chambers, positional changes, blockade of the bundle branches.
ProngR .Displays the spread of excitation throughout the myocardium of both ventricles. This wave is positive, and its height does not exceed 20 mm in the limb leads, and 25 mm in the chest leads. The height of the R wave is not the same in different leads. Normally, it is greatest in lead II. In ore leads V 1 and V 2 it is low (because of this it is often denoted by the letter r), then it increases in V 3 and V 4, and in V 5 and V 6 it decreases again. In the absence of the R wave, the complex takes on the appearance of QS, which may indicate transmural or cicatricial myocardial infarction.
Prong S. Displays the passage of the impulse through the lower (basal) part of the ventricles and the interventricular septum. This is a negative tooth and its depth varies widely, but should not exceed 25 mm. In some leads the S wave may be absent.
T wave. The final section of the ECG complex, displaying the phase of rapid ventricular repolarization. In most leads this wave is positive, but it can also be negative in V1, V2, aVF. The height of the positive waves directly depends on the height of the R wave in the same lead - the higher the R, the higher the T. The causes of a negative T wave are varied - small focal myocardial infarction, dishormonal disorders, previous meals, changes in the electrolyte composition of the blood, and much more. The width of the T waves usually does not exceed 0.25 ms.
Segment S-T– the distance from the end of the ventricular QRS complex to the beginning of the T wave, corresponding to full coverage of the ventricles by excitation. Normally, this segment is located on the isoline or deviates from it slightly - no more than 1-2 mm. Large S-T deviations indicate a severe pathology - a violation of the blood supply (ischemia) of the myocardium, which can lead to a heart attack. Other, less serious reasons are also possible - early diastolic depolarization, a purely functional and reversible disorder mainly in young men under 40 years of age.
Interval Q-T– the distance from the beginning of the Q wave to the T wave. Corresponds to ventricular systole. Magnitude interval depends on heart rate - the faster the heart beats, the shorter the interval.
ProngU . An unstable positive wave, which is recorded after the T wave after 0.02-0.04 s. The origin of this tooth is not fully understood, and it has no diagnostic value.
ECG interpretation
Heart rhythm . Depending on the source of generation of impulses of the conduction system, sinus rhythm, rhythm from the AV junction, and idioventricular rhythm are distinguished. Of these three options, only sinus rhythm is normal, physiological, and the other two options indicate serious disturbances in the conduction system of the heart.
A distinctive feature of sinus rhythm is the presence of atrial P waves - after all, the sinus node is located in the right atrium. With a rhythm from the AV junction, the P wave will overlap the QRS complex (while it is not visible, or follow it. With an idioventricular rhythm, the source of the pacemaker is in the ventricles. In this case, widened deformed QRS complexes are recorded on the ECG.
Heart rate. It is calculated by the size of the gaps between the R waves of neighboring complexes. Each complex corresponds to a heartbeat. It is not difficult to calculate your heart rate. You need to divide 60 by the R-R interval, expressed in seconds. For example, the R-R gap is 50 mm or 5 cm. At a belt speed of 50 m/s, it is equal to 1 s. Divide 60 by 1 to get 60 heart beats per minute.
Normally, heart rate is in the range of 60-80 beats/min. Exceeding this indicator indicates an increase in heart rate - tachycardia, and a decrease - a decrease in heart rate, bradycardia. With a normal rhythm, the R-R intervals on the ECG should be the same, or approximately the same. A small difference in R-R values is allowed, but not more than 0.4 ms, i.e. 2 cm. This difference is typical for respiratory arrhythmia. This is a physiological phenomenon that is often observed in young people. With respiratory arrhythmia, there is a slight decrease in heart rate at the height of inspiration.
Alpha angle. This angle displays the total electrical axis of the heart (EOS) - the general direction vector of electrical potentials in each fiber of the conduction system of the heart. In most cases, the directions of the electrical and anatomical axis of the heart coincide. The alpha angle is determined using the six-axis Bailey coordinate system, where standard and unipolar limb leads are used as axes.
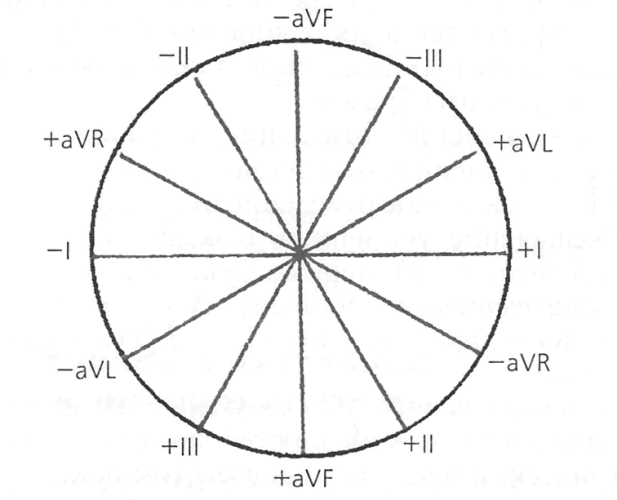
Rice. 8. Six-axis coordinate system according to Bailey.
The alpha angle is determined between the axis of the first lead and the axis where the largest R wave is recorded. Normally, this angle ranges from 0 to 90 0. In this case, the normal position of the EOS is from 30 0 to 69 0, the vertical position is from 70 0 to 90 0, and the horizontal position is from 0 to 29 0. An angle of 91 or more indicates a deviation of the EOS to the right, and negative values of this angle indicate a deviation of the EOS to the left.
In most cases, a six-axis coordinate system is not used to determine EOS, but is done approximately by the value of R in standard leads. In the normal position of the EOS, the height of R is greatest in lead II and smallest in lead III.
Using an ECG, various disorders of the rhythm and conduction of the heart, hypertrophy of the heart chambers (mainly the left ventricle), and much more are diagnosed. ECG plays a key role in diagnosing myocardial infarction. Using a cardiogram, you can easily determine the duration and extent of a heart attack. Localization is judged by the leads in which pathological changes are detected:
I – anterior wall of the left ventricle;
II, aVL, V 5, V 6 – anterolateral, lateral walls of the left ventricle;
V 1 -V 3 – interventricular septum;
V 4 – apex of the heart;
III, aVF – posterodiaphragmatic wall of the left ventricle.
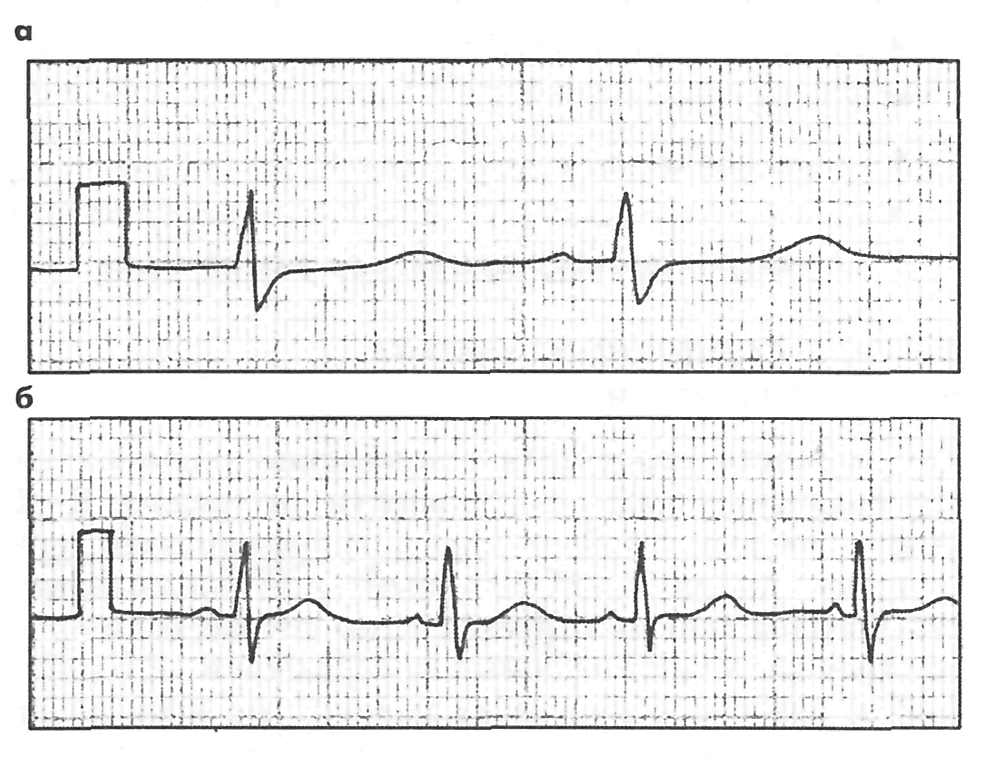
ECG is also used to diagnose cardiac arrest and evaluate the effectiveness of resuscitation measures. When the heart stops, all electrical activity stops, and a solid isoline is visible on the cardiogram. If resuscitation measures (indirect cardiac massage, administration of drugs) are successful, the ECG again displays waves corresponding to the work of the atria and ventricles.
And if the patient looks and smiles, and the ECG shows an isoline, then two options are possible - either errors in the ECG recording technique, or a malfunction of the device. The ECG is recorded by a nurse, and the data obtained is interpreted by a cardiologist or a functional diagnostics doctor. Although a doctor of any specialty is required to navigate issues of ECG diagnostics.
To determine the diagnosis, one of the most indispensable aids to a doctor is a cardiogram. It can help identify important heart diseases such as myocardial infarction or arrhythmia. And at the same time, it is inexpensive and accessible to everyone, and the method of its construction is based on a careful study of the bioelectrical activity of the heart muscles. Now we will teach anyone to read a cardiogram.
1.
When recording an ECG, it is important to avoid all kinds of interference and guidance currents; the minivolt should not exceed ten millimeters
2.
Heart rhythm is determined by the frequency of heart contractions and their regularity, conductivity and the source of excitation are determined. This is determined by comparing the duration of the R-R intervals. If the heart rate rhythm is correct, this is calculated by dividing 60 by the second-by-second interval R-R.

3.
The algebraic axis of the heart is calculated by determining the sum of the amplitudes of the QRS waves at any limb lead points.
4.
Carefully examine the atrial scar R. Measure its amplitude along the isoline from the top of the wave; it should be no more than twenty-five millimeters. Measure the distance from start to finish; if the person is healthy, it will not exceed 0.1 second.
5.
The PQ interval is an indicator of the speed of impulse delivery from the atrium to the ventricles. Its interval should be between 0.12 and 0.1 seconds. You also need to analyze the ventricular QRS complex, measuring the amplitude of the complex and the duration of each of its teeth.

6. Analyze the T wave. It reflects the relaxation phase of the heart muscle. It is necessary to determine its polarity, amplitude and shape. When a person is healthy, this wave is positive and has the same polarity as the wave responsible for the ventricular complex. Its shape should be gently ascending and have a steeply descending knee.
MINISTRY OF HEALTH OF THE RF |
|||||||||||||||||||||||||||||||||||
NIZHNY NOVGOROD STATE |
|||||||||||||||||||||||||||||||||||
MEDICAL INSTITUTE |
|||||||||||||||||||||||||||||||||||
A.V. SUVOROV |
|||||||||||||||||||||||||||||||||||
Publishing house NGMI NIZHNY NOVGOROD, 1993
Kyiv – 1999
UDC 616.12–008.3–073.96
Suvorov A.V. Clinical electrocardiography. – Nizhny Novgo-
genus. Publishing house NMI, 1993. 124 p. Ill.
The book by Suvorov A.V. is a good, complete textbook for cardiologists, therapists and senior students of medical institutes on all sections of electrocardiography. The features of ECG recording, normal ECG in standard and unipolar leads, all types of atrioventricular blocks, bundle branch blocks, ECG features in hypertrophies, conduction disorders, arrhythmias, myocardial infarction, ischemic heart disease, thromboembolism, cerebrovascular accidents, etc. are described in detail.
Published by decision of the editorial and publishing council of NMI
Scientific editor Professor S. S. BELOUSOV
Reviewer Professor A. A. OBUKHOVA
ISBN 5-7032-0029-6
© Suvorov A.V., 1993
PREFACE
Electrocardiography is one of the informative and most common methods of examining patients with heart disease. An ECG also makes it possible to diagnose diseases and syndromes that require emergency cardiac care, and above all myocardial infarction, paroxysmal tachyarrhythmias, conduction disorders with Morgagni–Edams–Stokes syndrome, etc. The need for their diagnosis arises at any time of the day, but, unfortunately, interpretation ECG presents significant difficulties for many doctors, and the reason for this is poor study of the method at the institute, and the lack of courses on ECG diagnostics at advanced training faculties for doctors. It is very difficult to acquire literature on clinical electrocardiography. The author sought to fill this gap.
The manual on electrocardiography is structured traditionally: first, the electrophysiological foundations of electrocardiography are briefly outlined, the section of a normal ECG in standard, unipolar and chest leads, and the electrical position of the heart are presented in detail. The section “ECG for myocardial hypertrophy” describes general signs and criteria for atrial and ventricular hypertrophy.
When describing rhythm and conduction disorders, the pathogenetic mechanisms of the development of syndromes, clinical manifestations and medical tactics are presented.
The sections on ECG diagnosis of coronary artery disease, especially myocardial infarction, as well as infarction-like diseases, which are of great importance for practice, are covered in detail.
For complex ECG syndromes, a diagnostic search algorithm has been developed to facilitate the diagnosis of pathology.
The book is intended for doctors who want to study the theory and practice of this important area of cardiology on their own or with the help of a teacher in a short time.

1. TECHNIQUE FOR REMOVING ELECTROCARDIOGRAM
The electrocardiogram is recorded using electrocardiographs. They can be single-channel or multi-channel. All electrocardiographs (Fig. 1) consist of an input device (1), an amplifier of cardiac biopotentials (2) and a recording device (3).
The input device is a lead switch with cables of different colors extending from it.
The amplifiers have a complex electronic circuit that allows them to enhance the biopotentials of the heart several hundred times. The power source for the amplifier can be batteries or AC power. For safety reasons when working with an electrocardiograph and to prevent interference, the device must be grounded using a wire, one end of which is attached to a special terminal of the electrocardiograph, and the other to a special circuit. If this is not available, in emergency cases, central heating water pipes can be used for grounding (as an exception).
The recording device converts electrical vibrations into mechanical ones. Mechanical pen recording is carried out using ink or carbon paper. Recently, thermal recording has become widespread.
The point is that a feather heated by electric current melts the fusible layer of the tape, exposing the black base.
To record an ECG, the patient is placed on a couch. To obtain good contact, gauze pads moistened with saline are placed under the electrodes. Electrodes are applied to the inner surfaces of the lower third of the upper and lower extremities, a red cable is connected to the right arm, a black cable (patient grounding) to the right leg, a yellow cable to the left arm and a green cable to the left lower extremity. The pear-shaped chest electrode with a suction cup is connected to a white cable and installed in specific positions on the chest.
ECG recording begins with a reference millivolt, which should be equal to 10 mm.
IN 12 leads are recorded without fail - three standard, three unipolar and six chest leads, III, avF leads should preferably be taken in the inhalation phase. Additional leads are recorded according to indications.
IN Each lead should record at least 5 QRS complexes; for arrhythmias, one of the leads (II) is recorded on a long tape. The standard recording speed is 50 mm/sec; for arrhythmias, a speed of 25 mm/sec is used to reduce paper consumption. The voltage of the QRS complexes can be increased and decreased by 2 times depending on the research task.
An application for an ECG study is written on a special form or in a journal, which indicates the full name, gender, blood pressure, age of the patient, and diagnosis. It is imperative to report any medications you are taking.
therapy with cardiac glycosides, β-blockers. diuretics, electrolytes, antiarrhythmic drugs of the quinidine series, rauwolfia, etc.
2. ELECTROPHYSIOLOGICAL BASICS OF ELECTROCARDIOGRAPHY
The heart is a hollow muscular organ divided by a longitudinal septum into two halves: the left arterial and the right venous. The transverse septum divides each half of the heart into two sections: the atrium and the ventricle. The heart performs certain functions: automaticity, excitability, conductivity and contractility.
Automaticity is the ability of the conduction system of the heart to independently produce impulses. To the greatest extent the function
The sinus node (the center of first-order automaticity) has automaticity. At rest, it produces 60–80 impulses per minute. In case of pathology, the source of rhythm can be the atrioventricular node (the center of second-order automaticity); it produces 40–60 impulses per minute.
The conduction system of the ventricles (idioventricular rhythm) also has an automatic function. However, only 20–50 impulses are generated per minute (third-order center of automaticity).
Excitability is the ability of the heart to respond by contraction to internal and external stimuli. Normally, excitation and contraction of the heart occur under the influence of impulses from the sinus node.
Impulses can be not only nomotopic (from the sinus node), but also heterotopic (from other parts of the conduction system of the heart). If the heart muscle is in a state of excitation, it does not respond to other impulses (absolute or relative refractory phase). Therefore, the heart muscle cannot be in a state of tetanic contraction. When the myocardium is excited, an electromotive force appears in it in the form of vector quantities, which is recorded in the form of an electrocardiogram.
Conductivity. Having originated in the sinus node, the impulse propagates orthograde through the atrial myocardium, then through the atrioventricular node, the His bundle, and the ventricular conduction system. The intraventricular conduction system includes the right branch of the His bundle, the main trunk of the left branch of the His bundle and its two branches, anterior and posterior, and ends with the Purkinje fibers, which transmit impulses to the cells of the contractile myocardium (Fig. 2).
The speed of propagation of the excitation wave in the atria is 1 m/sec, in the ventricular conduction system 4 m/sec, and in the atrioventricular node 0.15 m/sec. Retrograde impulse conduction is sharply slowed down, atrioventricular delay allows the atria to contract before the ventricles. The most vulnerable areas of the conduction system are: atrioventricular node with AV delay, right bundle branch, left anterior branch,
As a result of the impulse, the process of excitation (depolarization) of the myocardium begins at the beginning of the interventricular septum, right and left ventricles. Excitation of the right ventricle may begin earlier (0.02"") than the left. Subsequently, depolarization captures the myocardium of both ventricles, and the electromotive force (total vector) of the left ventricle is greater than the right one.

th. The process of depolarization proceeds from the apex to the base of the heart, from the endocardium to the epicardium.
The process of recovery (repolarization) of the myocardium begins at the epicardium and spreads to the endocardium. During repolarization, a significantly lower electromotive force (EMF) occurs than during depolarization.
The process of depolarization and repolarization of the myocardium is accompanied by bioelectric phenomena. It is known that the protein-lipid membrane of the cell has the properties of a semi-permeable membrane. K+ ions easily penetrate through the membrane and phosphates, sulfates, and proteins do not penetrate. Since these ions are negatively charged,

they attract positively charged K+ ions. The concentration of K+ ions inside the cell is 30 times higher than in the extracellular fluid. Nevertheless, negative charges predominate on the inner surface of the membrane. Na+ ions are located predominantly on the outer surface of the membrane, because the cell membrane at rest is poorly permeable to Na+. The Na+ concentration in the extracellular fluid is 20 times higher than inside the cell. The cell potential at rest is approximately
but 70–90 mV.
When the myocardium is depolarized, the permeability of cell membranes changes, sodium ions easily penetrate the cell and change the charge of the inner surface of the membrane. Due to the fact that Na+ enters the cell, the electrical charge on the outer surface of the membrane changes. Depolarization changes the charge on the outer and inner surfaces of cell membranes. The potential difference that occurs during excitation is called the action potential, it is about 120 mV. During the process of repolarization, K+ ions leave the cell and restore the resting potential. Upon completion of repolarization, Na+ is removed from the cell into the extracellular space using sodium pumps, and K+ ions actively penetrate into the cell through the semi-permeable cell membrane (Fig. 3).
The repolarization process proceeds more slowly than depolarization and causes less emf than the excitation process.
Repolarization begins in the subepicardial layers and ends in the subendocardial layers.
The process of depolarization in a muscle fiber is more complex than in an individual cell. The excited area is charged negatively in relation to the area at rest, and dipole charges are formed, equal in magnitude and opposite in direction. If a dipole with a positive charge moves towards the electrode, a positively directed tooth is formed, if from the electric

troda – negatively directed.
The human heart contains many muscle fibers. Each excited fiber represents a dipole. Dipoles move in different directions. The sum of the vectors of muscle fibers of the right and left ventricles is written as a scalar quantity
– electrocardiograms.
IN In each lead, the ECG curve represents the sum of the vectors of the right and left ventricles and atria (biocardiogram theory).
3. NORMAL ECG IN STANDARD LEADS
IN At the beginning of the 20th century, Einthoven proposed standard leads. Einthoven presented the human body in the form of an equilateral triangle. The first standard lead registers the difference in potentials of the right and left hands, the second – the difference in potentials of the right hand and left leg, the third – the difference in potentials of the left hand and left leg. According to Kirchhoff's law, the second lead represents the algebraic sum of the first and third leads. All elements of the electrocardiogram obey this rule. The first lead reflects the potentials of the subepicardial surface of the left ventricle, the third – the potentials of the posterior wall of the left ventricle and the subepicardial surface of the right ventricle.
A normal ECG in standard leads is represented by a series of waves and intervals, designated by Latin letters (Fig. 4). If the amplitude of the tooth is more than 5 mm, it is indicated by a capital letter, if less than 5 mm, then by a small letter.
Wave P - this atrial complex consists of a hollow ascending limb and a symmetrically located descending limb, which are connected by a rounded apex. The duration (width) of the tooth does not exceed 0.08-0.1 seconds (1 mm - 0.02 ""), the height P is 0.5-2.5 mm. The largest amplitude P in
second standard lead. Normally PII >PI >PIII. PI >0.l"" indicates hypertrophy of the left atrium; with PIII >2.5 mm we can speak of hypertrophy of the right atrium. The duration of the P wave is measured from the beginning of the ascending to the end of the descending knee, the amplitude

P - from the base of the tooth to its top.
Interval PQ (R) – from the beginning of P to the beginning of g or R. It corresponds to the time of passage of the impulse through the atria, through the atrioventricular node, along the His bundle, bundle branches, and Purkinje fibers.
The duration of the PQ interval normally fluctuates 0.12"÷ 0.20"" and depends on the pulse rate. Prolongation of the PQ interval is observed when atrioventricular conduction is impaired; shortening of PQ is associated with a sympatheticoadrenal reaction, premature ventricular excitation syndrome, atrial or nodal pacemaker, etc.
Segment PQ – located from the end of P to the beginning of Q (R). The ratio of P to the PQ segment is called the Makruz index, its norm is 1.1–1.6. An increase in the Macruse index indicates hypertrophy of the left atrium.
The QRS complex reflects the process of ventricular depolarization, measured in the second standard lead from the beginning of Q to the end of S, the normal duration is 0.05–0.1 "". QRS prolongation is associated with myocardial hypertrophy or intraventricular conduction disturbances.
The Q wave is associated with the excitation of the interventricular septum (optional, with a negative amplitude). The duration of Q in the first and second standard leads is up to 0.03"", in the third standard lead - up to 0.04". The amplitude of Q is normally no more than 2 mm or no more than 25% R. Widening of Q and its increase indicate the presence of focal changes in the myocardium.
The R wave is caused by ventricular depolarization, has an ascending limb, an apex, and a descending limb. The time from Q (R) to the perpendicular from the apex of R indicates an increase in the rate of depolarization of the ventricles and is called the time of internal deviation, for the left ventricle no more than 0.04"", for the right - 0.035"". Serration R